In my book, Measuring Difference, numbering normal: setting the standards for disability in the interwar period, I show how specific conceptions of normalcy and disability emerged in the interwar period. The First World War necessitated new ways of thinking about and compensating for the disabled body and in the interwar period we see the solidification of disability as a distinct category. As other historians have identified, the interwar period is notable for societal focus on fitness, beauty, youth, and regeneration. There was a new national mood focused on a ‘return to normal’. This pursuit of normalcy connected with and reinforced concerns about health and disability, newly visible to the public eye. A host of biopolitical processes combined to make disability visible, measurable and quantifiable.
Through this process, the older debates that defined degenerative traits as heritable or deterioration as resulting from moral failing shifted and were reframed under the aegis of disability and scientific studies—especially those focused on measurement.A good example of how this kind of discourse filtered out to the public can be seen in a 1925 article from Cosmopolitan magazine, in which the author attempted to reassure readers whose weight varied from the ‘normal’ number prescribed in Army and Insurance charts
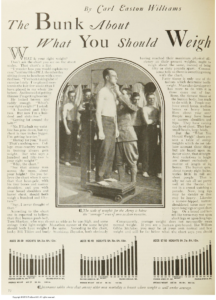
Examples from Cosmopolitan Magazine 1925. Striving for normalcy Carl Easton Williams ‘The Bunk About What You Should Weigh’ Cosmopolitan (New York, 1925): 72-73, 241
As the columnist explained, the conflation of the average with the normal obscured the true variability of the human body. I open my book by using the example of the BMI scale to argue that measures that are easy to calculate and compare tend to be privileged, thus distorting our understanding of normalcy. For instance, the first person to argue that there was an ideal weight that corresponded to height (Adolphe Quetelet) deliberately excluded those he deemed not ‘fully developed’ or ‘well-formed’ from his data.[i] This demonstrates firstly, how pre-existing biases are reinforced and amplified by seemingly objective technologies. Secondly, it demonstrates how excluding disabled individuals from relevant datasets artificially elevates the standard of ‘normalcy’. As historians of technology have demonstrated, standards tend to perpetuate themselves and to become increasingly opaque as they do so. Yet such standards exert a powerful influence on the way we understand the body through measurement and quantification.
A central tenet of disability studies is that disability varies dependent on context, time-period, and society, as well as varying with the individual and their community. Measuring Difference, numbering normal shows that disability is also dependent on measurement systems. This was especially true historically in cases of invisible but experiential disability such as hearing loss and breathlessness, which required new tools and ideally new instruments to become visible and quantifiable in the interwar period. I use the examples of the audiometer and the spirometer to show how this process developed in the cases of hearing loss and respiratory disability. By focusing on the creation of the data on which the standards of these instruments rest, it is possible to evaluate how the normal body is defined prima facie, and by doing so highlight the existence of a ‘disability data gap’, especially relevant to our understanding of compensation for acquired disability. In this way, I demonstrate another central tenet of disability studies, that disability, is always connected to power. As a result, the experience of disability is intersectional. Like the pandemic, disability has the potential to impact on individuals regardless of their social category. Yet not everyone experiences it equally. How a body is classified or experienced as normal or pathological reveals not just what matters to us but who matters to us.
Women in history have been made meaningful through the efforts of a generation of historians who have (and continue to) work in innovate ways to reveal previously concealed histories. I continue in this tradition by highlighting the ways in which women matter to disability history. For instance, chapter three, ‘The artificial ear and the disability data gap’ focuses on the development of the Post Office’s Artificial Ear technology, which the Post Office engineering department designed to provide a minimum standard of normal hearing for testing telephone transmission. As the standard was set through gathering data from just ‘ten normal male’ ears, I demonstrate that the standard of normal hearing was set artificially high. Then, in chapter four, ‘The audiometer and the medicalisation of hearing loss’, I suggest that the Post Office’s exclusion of women from their data sets and design remits led to a failed product (a telephone adaptor to link the telephone to the NHS Medresco hearing aid). By designing a prosthetic that was impossible for women who chose to conceal their hearing aids to use, the engineers neglected to account for the social aspects of hearing loss, which was particularly harmful to women.
In part two of my book, which is concerned with respiratory disability, I start chapter five ‘The spirometer and the normal subjects’ by exploring the difficulties involved in separating biological features presumably related to sex from gendered features related to living as a woman in society. For instance, the gendered imperative to conceal a prosthetic or to embody an idealised figure. In the section ‘breathing like a girl’, I explore ideas about gendered habits like costal breathing by tracking how the normal values used in spirometry to assess lung function in women changed from the nineteenth to the twentieth century. Consider how breathing in to hold in the stomach affects breathing.Then imagine how wearing a corset would have affected your lung function measurements. The impact of these gendered habits blurred the boundaries between gender and sex for scientists who then linked feminine ‘costal’ breathing with civility and racial purity. As this example shows, attempts to define the standard of normalcy for certain groups also entailed defining the relevant groups for measurement in the first place. These normalisation processes then had a corresponding impact on the classification of disability.
Untangling these different disabling classification systems necessitates studying women’s history alongside other relevant social categories such as race and class. We need to approach disability history through an intersectional framework because disability is always connected to power. By considering these social categories in connection to each other rather than in isolation, we can make this power visible, measurable, and accountable.
Coreen McGuire is Lecturer in Twentieth-Century British History at Durham University. Her first book, Measuring Difference, Numbering Normal: Setting the standards for disability in the interwar period combines history of medicine, science and technology studies, and disability history. She won the Disability History Association prize for outstanding article in 2020 and is currently working on a co-authored book project on British scientist Dr Phyllis Kerridge’s contributions to science in Britain with Dr Jaipreet Virdi for Johns Hopkins Press.
i] Adolphe Queelet, A treatise on man and the development of his faculties (1842 trans. Edinburgh, William and Robert Chambers) org.1835 p.67 Quetelet came up with the concept of BMI but the term was coined by Ancel Keys.